1.3.JPG.d62b3dcb83ab05b18608cab875c00b38.JPG.0bc6abddd86cd947ae248677b66345a5.JPG)
Emerald ash borer doesn't just kill ash trees - it also kills humans

Entry posted by Kveldssanger
6,809 views
The presence of trees in the urban environment is certainly beneficial for the health and well-being of local residents, who will, generally-speaking, benefit more than they suffer as a result of the trees’ presence. Somewhat anecdotally, it has also been shown that it is the presence of healthy trees that has such beneficial impacts. In this sense, if tree populations suffer at the hands of a biotic or abiotic stressor, visibly decline in health, and potentially die in time (even on a massive scale), then the impact will also be ‘felt’ by the local residents.
As a means of adding weighting to this statement, we can look at a US-based study that assessed whether the presence of the tree pest emerald ash borer (Agrilus planipennis), as it ravaged urban ash (Fraxinus spp.) populations, brought about adverse health responses in humans as well. The beetle has spread quite rapidly in the US since its arrival in 2002, and now occupies an area of land quite massive in scale (as shown by the map below). Specifically, the study looked at whether the presence of emerald ash borer had associations with the rate of mortality caused by cardiovascular and lower-respiratory-tract issues. The authors of this study selected these causes of death, because they are the first and third highest causes of death, respectively. Furthermore, there is reason to suggest that these two causes of death can be influenced by the presence (or lack) of trees.
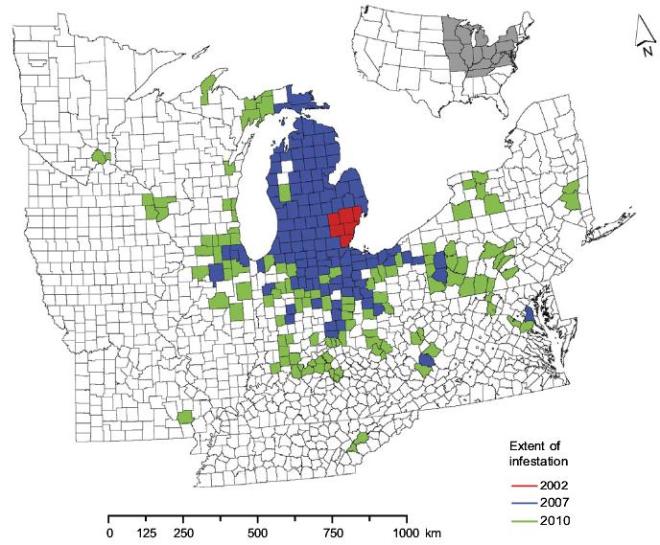
A map of where the emerald ash borer has been found in the USA, on a county level.
In all of the US states that had at least one case of the emerald ash borer, the authors analysed information, from 1990-2007, outlining the cause of death for citizens. With this data, the authors looked at whether the presence of the beetle, and how long it had existed in a state, had any influence upon the mortality rates associated with the two causes of death mentioned. These comparisons were then related to the estimated abundance of ash trees in the states, and demographic data obtained via census records.
Following on from data analysis, the authors identified that the presence of the beetle had a more significant impact upon respiratory-related mortality rates in wealthier counties (where there was a greater access to ash trees, compared to poorer counties) and, on average, there were 6.8 more deaths per 100,000 individuals in states host to the pest than prior to the state’s date of infestation. However, the impact of its presence increased over time, therefore meaning that areas that have been infested for longer will experience a higher average mortality rate than those areas more recently infected (as can be seen in the below table). At the time of the study, the authors therefore estimated that 6,113 respiratory-related human deaths had been caused by the presence of the emerald ash borer between 2002-2007, because of its impact upon its host ash trees (which almost always will die, or are cut down upon detection of them being infected). Therefore, we can perhaps observe that dying trees (and an increasing lack of trees) means dying humans. However, the fact that there is an anticipated 2-5 year lag associated with beetle presence and human mortality rates, the real effects of the ash borer upon human health may not yet be fully appreciated. Curiously, the authors also suggest that the media coverage of the ash borer’s presence may induce stress in some individuals, and such stress may potentially exacerbate (or create) health issues. Perhaps this highlights the emotional relationship people have with trees, and at times there may even be a sort of cross-kingdom empathy (and associated grief).

The impact upon respiratory-related human mortality rates caused by the emerald ash borer.
The observed impacts upon cardiovascular-related mortality rates per 100,000 individuals was even higher. In counties host to the emerald ash borer, an additional 16.7 deaths per 100,000 can be attributed to the pest’s presence. Therefore, 15,080 deaths can be directly linked to the effects of the borer, meaning that a total of 21,193 individuals have suffered mortality, between 2002-2007. Much like with respiratory-related deaths, the duration of time for which the beetle has been present has an impact upon the rate of mortality (see the below table). It was also found that individuals in counties with moderate levels of average income were most markedly affected.

The impact upon cardiovascular-related human mortality rates caused by the emerald ash borer.
Not provided in the journal, I decided to plot both sets of figures relating to the mortality rate increase observed with the presence of the borer, and assess the two lines (as shown below). What we can crudely see is that, as the years progress, the dispiraity increases between the two data sets, in favour of cardiovascular-related deaths. However, respiratory-related deaths consistently remain, across the six year period, 39-41% lower than cardiovascular-related deaths. Therefore, enriching cardiovascular health may likely be a more significant focal point with regards to any mitigation measures that may take place, though we must obviously be aware that there is likely going to be a levelling-off threshold, by where no more ash trees exist and therefore the mortality rate cannot suffer any further (accompanied by lag times). During this time, re-planting may of course occur, and offset any adverse impacts associated with ash mortality. Of course, these new trees will take time to mature, and therefore it may be many decades before health impacts begin to markedly reverse.

Comparing the two data sets (blue line: cardiovascular mortality rates; orange line: respiratory mortality rates).
There is no question that such data is indeed very interesting, and the results don’t necessarily remain limited to the emerald ash borer. Across the world, we can observe trees dying or being removed because of pest or disease outbreaks, so one can suspect that similar impacts may be associated with, for example, ash removal because of ash dieback, elm removal because of Dutch elm disease, or tree removal caused by Xylella fastidiosa. Granted, the actual impacts may differ (either be more severe, or less severe), though there will certainly be impacts. The findings that more affluent individuals were more adversely impacted by the emerald ash borer is very interesting, though perhaps not surprising, as environmental inequality certainly exists within urban districts (with more affluent areas having a more abundant tree presence). In this sense, less affluent neighbourhoods may already be suffering as a result of other stressors, and the lack of ash trees in the near locality means that they simply aren’t impacted by their death, because they are not directly experiencing such significant tree mortality. Other socio-demographic issues may also be implicated in this equation, such as the highest level of education an individual has. Similarly, the reduction is ecosystem sevices (pollution removal, encouragement to exercise outdoors, and so on) associated with the death of ash trees may have an impact upon respiratory and cardiovascular health, and this impact will be most pronounced where the most trees have been lost, which is (in this case) in the more affluent areas.

ATTENTION: Have you seen this pest? It is wanted for the death of over some 100,000,000 ash trees, in the USA. Source: Aetree.
Source: Donovan, G., Butry, D., Michael, Y., Prestemon, J., Liebhold, A., Gatziolis, D., & Mao, M. (2013) The relationship between trees and human health: evidence from the spread of the emerald ash borer. American Journal of Preventive Medicine. 44 (2). p139-145.



{kind=link}
0 Comments
Recommended Comments
There are no comments to display.
Create an account or sign in to comment
You need to be a member in order to leave a comment
Create an account
Sign up for a new account in our community. It's easy!
Register a new accountSign in
Already have an account? Sign in here.
Sign In Now